
In brief, AV nodal blocks are when there is a fault in the AV node releasing the electrical impulse which responsible for ventricular contraction. Sometimes it is an SA/AV delay, and sometimes it is a complete mismatch, and the difference is how we categorise them. They can be caused by issues with electrical conduction, physical/ structural damage, or may be a normal finding for the patient. It is likely to stimulate bradycardia, which is results in decreased poor cardiac output and poor haemodynamic state.
Visual images and representations here… no ideal who to credit them to
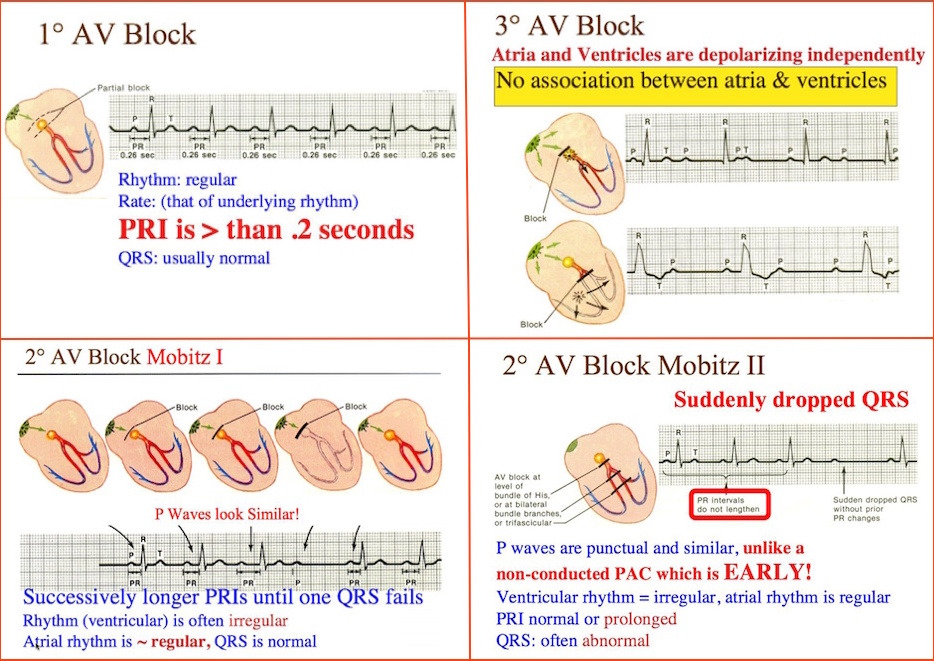
A first degree block is a conduction delay of over 0.20 seconds. That is, more simply, five small squares between the end of the P wave and the start of the QRS complex.
First degree blockages are normal in 1% of the young adult population, or in those with increased vagal tone. In the elderly, it’s often a sign of medications such as digoxin (digitalis) or previous MI.
However, more sinister causes exist. The SA node is usually fed by the right coronary artery (RCA), or left circumflex (LCx) artery, which usually sits in the lateral aspects of the heart. Infarct or ischaemia to the LCx causes poor perfusion and thus poor performance. These are often found in inferior MI, but could be present in any AMI context.
As far as medication goes, nodal blockers like digoxin, beta blockers, amiodarone all alter the electronic pathway within the heart, which could produce a delay. There’s no end treatment for a first degree block, as they don’t usually cause any haemodynamic compromise, and don’t usually progress any further. In the absence of other abnormal findings, a first degree block is often abnormal finding for patients, requiring no intervention.
Life in the fast lane on the subject… find your own way to LITFL on the other types through this link.
A second degree type one is a progressively lengthening PR interval which eventually drops a QRS complex before starting again. It is usually due to a reversible blockage or delay in AV conduction.
All the risk factors for a first degree block have the chance to develop further into a second degree block. If it isn’t the patient’s’ normal underlying rhythm, it would tend to indicate more dangerous causes which are developing, such as drug toxicity or AMI.
Sometimes second degree type one is a normal, benign finding. It’s not common for second degree blocks to cause compromise, but if they do it normally results in bradycardia. Local treatment protocols suggest bradycardia in the form of second degree blocks should be treated with atropine first, adrenaline infusion second, and with trans-cutaneous pacing in the final instance.
Atropine is likely to resolve the bradycardia from first and second degree blocks in the first instance. Atropine inhibits vagal tone which allows for increased heart rates… or, in English, atropine inhibits the system slowing the heart rate down, allowing the body to determine the heart rate it needs.
Adrenaline acts as a chronotrope, accelerating the heart rate. The combination of atropine and adrenaline is likely to resolve the issue in second degree type one due to the reversible nature of type one blocks.
A second degree type two (wenckebach) has selective impulse conduction. Some are impulses are allowed through the AV node normally, and some have delays. The ‘normal’ impulses often have an extended PRI.
Second degree type two is never a benign finding and should be treated as such. Second degree type two is usually a progressed type one, or a result of significant structural changes in the electrical pathways of the heart. It is not uncommon for patients to progress from a bundle branch block to a second degree type two.
Accordingly, second degree type two is less likely to respond to chemical responses and pacing is usually required to correct haemodynamic compromise. Local protocols still state the staggered atropine/adrenaline/pacing cascade should be taken in second degree type two.
Second degree type two blocks have a high chance of converting to a third degree block, and having the complications which are associated with them. Because they are usually due to a failure in the his/purkinje system definitive treatment tends to be an implanted pacemaker, normally with or without some kind of antiplatelet or anticoagulant to minimise side effects.
If there is a wide complex present, the ventricles are providing an inherent rate. A broad complex indicates structural defects and is unlikely to respond to chemical cardioversion. Anticoagulants are particularly important at this point because the increased irregularity in rate increases the risk of thrombus and stroke.
Third degree blocks have a complete SA/AV disassociation- the SA node discharges the impulse, and the AV node or the ventricles take over and discharge another impulse, completely disassociated from the initial P wave.
Third degree blocks aren’t good. They are usually the result of severe structural defects, in the same manner as second degree type two. Alternatively can be caused by the same things discussed for first degree blocks which have progressed through, causing progressive AV nodal fatigues.
Third degree blocks will ultimately require a pacemaker in the absence of treatment of an underlying cause. The prehospital treatment is likely to be pacing for the same reasons as discussed in second degree type two- it requires structural support, or preparing for treatment of sudden cardiac arrest. For the same reason, the in hospital therapy is likely to be an implanted pacemaker with antiplatelet/ anticoagulant therapy.
Treatment is dependent on two factors: patients level of cardiovascular compromise, and the underlying cause. There is no specific treatment prehospitally, we are actually treating cardiogenic shock secondary to bradycardia.
The American Heart Association suggests we lean towards treatment with pacing in the first instance of any second degree blocks, which goes against the somewhat ambiguous wording of local protocol. Wellington Free (3.11) encourages staff to establish whether the blockage is high or low in the conduction system and tailoring treatment, which is likely to be the principle conveyed in our guidelines
Recap
Cardiac output= stroke volume x heart rate
In first degree and second degree type one block we typically see a decreased rate, and in second degree type two and third degree we see significantly decreased rates AND decreased stroke volume due to poorly performing ventricles.
Prehospital providers should consider underlying causes of bradycardia (such as AMI, toxicity, hypoxia), and then treat accordingly. In the absence of an acute cause, treatment should be tailored towards managing compromise.
Referral should be based on a solid history and the impression of the scenario presented. The only safe assumption is that second degree type two and third degree blocks are new, and require prompt cardiology referral. Red flags would be trauma, syncope, polypharmacy, age over 65, or an abnormal neuro examination. If in doubt- refer through- a cardiology consult does no harm.
Talking Points
Corrections always welcome.
If you’ve got examples of pictures, lay them up, or email a picture of them to me at work to put them up. It’s always nice to have an idea of how they’d look on a LP15 to increase familiarity.
Complications seen from AV blockages?
Cool, they’ve got a block- what does it matter?
Why is it that patients with AV blocks in hospital is so much more concerning? No idea? Have a hint
Links and references:
A much more detailed discussion on how to diagnose, with quality sections I’ve skipped such as mimics, courtesy of renal and nephrology news
An advanced read up on AV dysfunction, including AVNRT, which is important when you’re dishing out amiodarone. Related: amiodarone is not as safe as the 70s made us believe
There is some work being done on how we can restore electrical conductivity in structurally damaged patients, but this isn’t even in human testing stages. More here.
American Heart Association (2005) Chapter 7.3: Management of Symptomatic Bradycardia and Tachycardia Guidelines for Cardiopulmonary Resusciattion and Emergency Cardiovascular Care 112 (24) doi: https://doi.org/10.1161/CIRCULATIONAHA.105.166558
Garcia, T., & Holtz, N. (2013) 12 Lead ECG: The Art of Interpretation. Jones & Bartlett: USA.
Wellington Free (2016) 3.11 Bradycardia Comprehensive Practice Guidelines.

{kind=link}
Wink….wink…..wenckeback
Slow….slower……dropped…..
LikeLiked by 1 person
2015 (2010) AHA Update puts less emphasis on TCP as a first line Tx for all 2nd and 3rd degree HBs. 2015 update recommends atropine as a first line Tx for all symptomatic bradycardia, and only says “Do not rely on atropine for 2nd or 3rd degree HB.”

AHA2015 update also says adrenaline infusion may be as effective as TCP and both are used as temporizing measures while the patient is prepared for transvenous pacing.
Also the cautious use atropine in the presence of acute coronary ischemia or MI is clearly stated, and this may be a good rationale for us to choose adrenaline infusion or TCP as both can be titrated more accurately and stopped quickly if required.
LikeLike
would you be able to post a link to the whole article, which discusses the changes? I’d like to amend the article appropriately but all I can find on the AHA website links back to the original research from which this was written…
LikeLike
stand down…. http://circ.ahajournals.org/content/122/18_suppl_3/S729.figures-only
LikeLike
Soooooo, finally after not being able to read it… when it’s specifically speaking of 2nd/3rd deg AVB…
1) “Atropine administration should not delay implementation of external pacing for patients with poor perfusion.”, likely because
2) “These bradyarrhythmias are not likely to be responsive to reversal of cholinergic effects by atropine and are preferably treated with TCP or b-adrenergic support as temporizing measures while the patient is prepared for transvenous pacing.”
Which leads me to conclude that what the 2010 article suggests is that although atropine should be the first line *drug* we should consider that it may not be the first line treatment. Atropine sits superior in the algorithm because the side effects are less, and if it doesn’t work, nothing happens. If it does work, patients and providers don’t need to be subjected to the issues of TCP. It should be the preferred treatment for this reason, but the recommendation should be having a very low threshold for changing therapies. Beta agonists definitely appear to have a place as the mechanism isn’t relying on changing AV conductivity, rather having a more global chronotropic effect.
Both articles make commentary that it’s unlikely for atropine to work and atropine administration “should not delay TCP” (2005) and the T2(2)AVB & T3 AVB bradycardias “are preferably treated with TCP” (2010) ..
BUT: there are very few studies directly comparing drug therapy vs TCP in the poorly perfused. It’s interesting we’re having this discussion because your article (section 8.3 (2010), and mine, section 7.3 (2005)) are both using the same 1977 research by Chadda which has severe limitations, namely that it only looked at post AMI patients…
LikeLiked by 1 person
Atropine comes in the plastic thing (pro term) which is easy to be drawn up and can be given very quickly. This practical aspect may be behind the rationale for atropine administration, as both adrenaline infusion and TCP, especially when Pt is conscious, takes time.
Nevertheless, it dose not change the priority of TCP when wide QRS complex causing compromise, so once again our CPG is pretty cleverly written, don’t you think?
LikeLike
Great work Andrew. Best way to learn is to try teaching others too eh!
Just the one error I picked up is the ‘Wenckeback’ is supposed tone Type (Mobitz) l.
LikeLike