And just another note for the sceptics dissing the value of learning the extra knowledge, Amal in his one of the lectures present the case of fatality as a result of haemorrhargic tamponade secondary to pericarditis which was caused by administration of clopidogrel.
Once again, impressive display of knowledge, and thank you for sharing your thoughts.
From the EM Alliance;
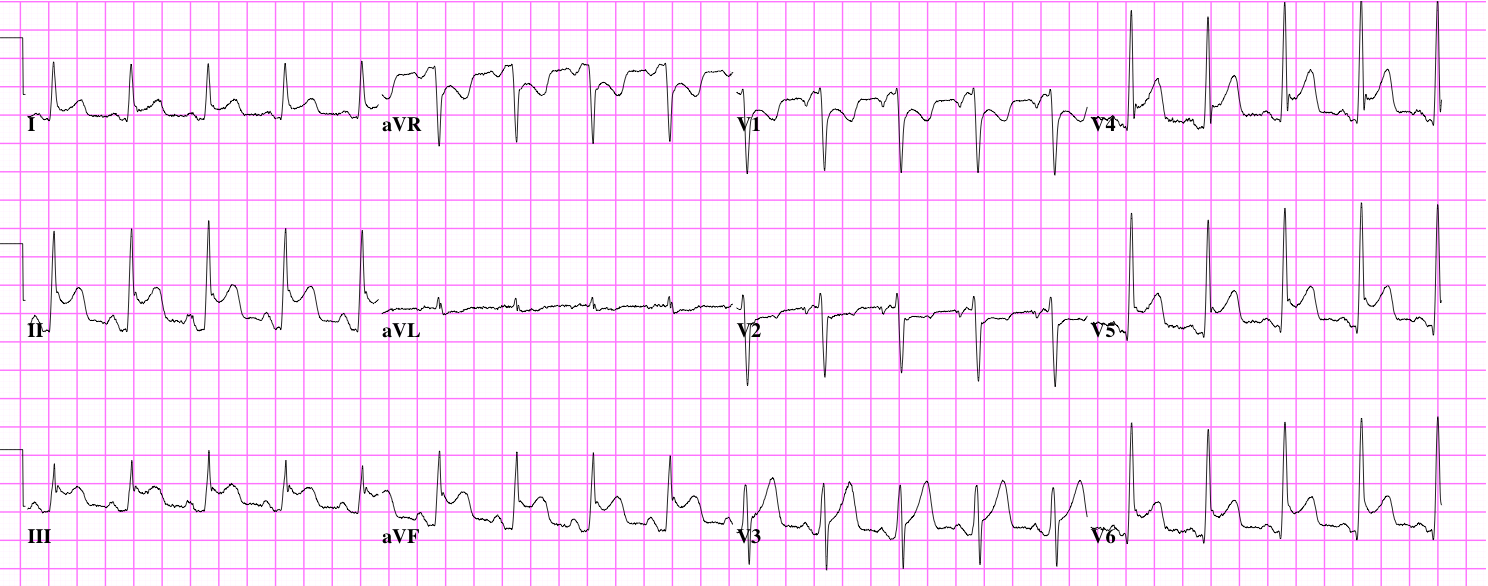
This Pt had pericarditis post 3 days of radiotherapy resulted in SOB and hypotension.
Pericarditis occurs globally over pericardium hence global ST elevation.
PR depression are usually seen in viral pericarditis but this is an example of exceptions.
Pericarditis resulted in pericardial effusion then tamponade causing haemodynamic instability.
As you know, I’m a big fan of Amal Mattu and his teaching is to “ALWAYS’;
1. Look at the Pt / clinical presentation may or may not include the characteristic chest pain (retrosternal, pleuritic, worse on lying flat, relieved by sitting forward), tachycardia and dyspnoea.
2. Rule out ACS before start digging for ST elevation mimics such as BER, Pericarditis.
Don’t go searching for pericarditis via global STE, PR depression etc as ACS can also present with PRD, it is often intermittent so may not be there.
Look for;
Reciprocal (any) ST depression (except for aVR or V1 as they are normal).
Flat, horizontal, or angry looking ST elevation (morphology/shape of ST elevation).
ST elevation in lead III>II
* If you see any of above, treat it as ACS/STEMI and don’t go any further down the list below.
Pericarditis/Myocarditis
No reciprocal ST-segment depression
Concave ST-segment morphology
STE in lead II > III
PR-segment depression (not specific)
Spodick’s sign = downward sloping of TP segment (not sensitive or specific)
I just realised that free Youtube clips of Amal’s old lectures are taken off and no longer viewable…
I highly recommend his ECG Weekly https://ecgweekly.com/mm-error/?code=100020
It costs only US$26 annually and really worth it!
looks pericarditis..ish with the widespread elevation, hx of lung CA might suggest a relationship between the two, along the lines of what Miriam was saying, the only thing with that would you see signs of right sided specific ischemia or damage, eg RBBB, hypertrophy . Awsum idea thanks for the invite!
Pericarditis/effusion: Hx of CA. Widespread ST elevation with no reciprocal changes, PRI depression. Lead II greater than Lead III, convex ST segments.
Wow, impressive level of knowledge displayed here and thank you all for taking time and being brave enough to share your knowledge, as that’s exactly what we are hoping to achieve!
I normally leave if for a block or two before uploading related FOAMs, as we don’t normally get this many comments (lol), but will try uploading something sooner this time.
It would also be good if you could comment on the reason for stabbing at the differencials so others can learn from your thought patterns. Cheers guys!
Yep I’ll go with early stage pericarditis (no flattening of ST segmant)
Slightly tachy
Widespread ST elevation with depression aVR and V1
ST morphology concave
Firstly, thank you Tatsu for the invite. Very cool idea to be hosting this forum.
The ST elevation appears too global to be related to STEMI (multiple coronary vessel involvement), coupled with the morphology of the segment would to me be more indicative of pericarditis. Additionally the global PR segment depression with reciprocal PR segment elevation in aVR would support this.
Rate/Rhythm: Sinus Tachycardia, Identical P waves with a 1:1 ratio with QRS, Normal PR interval
Axis: Normal axis
QRS: Narrow QRS, Normal QT
Morhology: Subtle Osbourne waves in I, II, III, AVF, V5, V6 with a more prominent one in V4. T wave inversion in V1 & V2, otherwise asymetrical and not peaked, widened or flattened.
STEMI Mimics: Morhpology indicative of LVH, no BBB, no pacing, no morphology consistent with hyperkalemia,
At a quick glance, it would appear to be a large Anteriolateral STEMI possibly involving multiple arteries (RAD, Circumflex, LAD or a combination of those) or a Circumflex occlusion only but with a dominant Circumflex reaching wide, however, to have such a large STEMI and be only c/o shortness of breath is a bit strange and the Osbourne waves are an interesting finding, the T wave
inversion could be a normal variant and the ST elevation doesn’t appear to be the typical convex shape.
The ST elevation is fairly widespread right through leads I, II, III, AVF, V3, V4, V5 and V6 and it is consistently concave with marked PR depression and AVR ST depression so there is a high index of suspicion for Pericarditis.
Another potential is benign early repolarisation. Again, widespread concave ST elevation, asymetrical T waves, and could also explain the osbourne waves however, there is reciprocal changes in AVR which don’t really seem consistent with BER and the ST elevation seems far too much to be BER but not able to rule out conclusively.
I’m going to put my money on Pericarditis but also unable to completely rule out STEMI or BER
Good on you for having a go at commenting on the ECG as it is obviously a still daunting thing to do despite we are doing our best to make this forum free from any negative criticism.
And yes, your interpretation is certainly one of the differencials.
Can you think of any other pathologies?
In terms of your obs re biphasic T waves, do you think the T waves on V1 deflect both positively and negatively across the isoelectric line?
Please encourage others to post their guess as I can guarantee that it will not cost their job or reputation, lol 😄
I’ll have a stab at it… the STE in inferior aspects naturally suggests RCA occlusion, and the STE in anterior lateral aspects suggest Cx occlusion.
Of note the biphasic T waves have an occlusion style pattern similar to De Winters or Wellens in V1.
Overall the ECG suggests to me there’s a current infarct to the inferior and lateral aspects, but is progressing into a full occlusion of both LAD and RCA.


And just another note for the sceptics dissing the value of learning the extra knowledge, Amal in his one of the lectures present the case of fatality as a result of haemorrhargic tamponade secondary to pericarditis which was caused by administration of clopidogrel.
LikeLike
Once again, impressive display of knowledge, and thank you for sharing your thoughts.
From the EM Alliance;
This Pt had pericarditis post 3 days of radiotherapy resulted in SOB and hypotension.
Pericarditis occurs globally over pericardium hence global ST elevation.
PR depression are usually seen in viral pericarditis but this is an example of exceptions.
Pericarditis resulted in pericardial effusion then tamponade causing haemodynamic instability.
As you know, I’m a big fan of Amal Mattu and his teaching is to “ALWAYS’;
1. Look at the Pt / clinical presentation may or may not include the characteristic chest pain (retrosternal, pleuritic, worse on lying flat, relieved by sitting forward), tachycardia and dyspnoea.
2. Rule out ACS before start digging for ST elevation mimics such as BER, Pericarditis.
Don’t go searching for pericarditis via global STE, PR depression etc as ACS can also present with PRD, it is often intermittent so may not be there.
Look for;
Reciprocal (any) ST depression (except for aVR or V1 as they are normal).
Flat, horizontal, or angry looking ST elevation (morphology/shape of ST elevation).
ST elevation in lead III>II
* If you see any of above, treat it as ACS/STEMI and don’t go any further down the list below.
Pericarditis/Myocarditis
No reciprocal ST-segment depression
Concave ST-segment morphology
STE in lead II > III
PR-segment depression (not specific)
Spodick’s sign = downward sloping of TP segment (not sensitive or specific)
LIFL also has a great info https://lifeinthefastlane.com/ecg-library/basics/pericarditis/
LikeLike
I just realised that free Youtube clips of Amal’s old lectures are taken off and no longer viewable…
I highly recommend his ECG Weekly https://ecgweekly.com/mm-error/?code=100020
It costs only US$26 annually and really worth it!
LikeLike
I have a copy of these if anyone wants them.
LikeLike
Jason, I hope your copy is not from the Workshop series I bought a couple of years ago…
LikeLike
No
LikeLiked by 1 person
looks pericarditis..ish with the widespread elevation, hx of lung CA might suggest a relationship between the two, along the lines of what Miriam was saying, the only thing with that would you see signs of right sided specific ischemia or damage, eg RBBB, hypertrophy . Awsum idea thanks for the invite!
LikeLiked by 1 person
Pericarditis/effusion: Hx of CA. Widespread ST elevation with no reciprocal changes, PRI depression. Lead II greater than Lead III, convex ST segments.
LikeLiked by 1 person
Concave not convex…Not enough coffee
LikeLike
Wow, impressive level of knowledge displayed here and thank you all for taking time and being brave enough to share your knowledge, as that’s exactly what we are hoping to achieve!
I normally leave if for a block or two before uploading related FOAMs, as we don’t normally get this many comments (lol), but will try uploading something sooner this time.
It would also be good if you could comment on the reason for stabbing at the differencials so others can learn from your thought patterns. Cheers guys!
LikeLike
Pericardial effusion and/or tamponade
LikeLiked by 1 person
Further investigation such as equal radial pulse pressure, muffled heart sounds and an elevated pulsus paradoxus would be supportive to this DX.
LikeLiked by 1 person
Yep I’ll go with early stage pericarditis (no flattening of ST segmant)
Slightly tachy
Widespread ST elevation with depression aVR and V1
ST morphology concave
LikeLiked by 1 person
Looks like a variant of takotsubo – broken heart syndrome
LikeLiked by 1 person
Firstly, thank you Tatsu for the invite. Very cool idea to be hosting this forum.
The ST elevation appears too global to be related to STEMI (multiple coronary vessel involvement), coupled with the morphology of the segment would to me be more indicative of pericarditis. Additionally the global PR segment depression with reciprocal PR segment elevation in aVR would support this.
LikeLiked by 1 person
OK I’ll give it a crack.
Rate/Rhythm: Sinus Tachycardia, Identical P waves with a 1:1 ratio with QRS, Normal PR interval
Axis: Normal axis
QRS: Narrow QRS, Normal QT
Morhology: Subtle Osbourne waves in I, II, III, AVF, V5, V6 with a more prominent one in V4. T wave inversion in V1 & V2, otherwise asymetrical and not peaked, widened or flattened.
STEMI Mimics: Morhpology indicative of LVH, no BBB, no pacing, no morphology consistent with hyperkalemia,
At a quick glance, it would appear to be a large Anteriolateral STEMI possibly involving multiple arteries (RAD, Circumflex, LAD or a combination of those) or a Circumflex occlusion only but with a dominant Circumflex reaching wide, however, to have such a large STEMI and be only c/o shortness of breath is a bit strange and the Osbourne waves are an interesting finding, the T wave
inversion could be a normal variant and the ST elevation doesn’t appear to be the typical convex shape.
The ST elevation is fairly widespread right through leads I, II, III, AVF, V3, V4, V5 and V6 and it is consistently concave with marked PR depression and AVR ST depression so there is a high index of suspicion for Pericarditis.
Another potential is benign early repolarisation. Again, widespread concave ST elevation, asymetrical T waves, and could also explain the osbourne waves however, there is reciprocal changes in AVR which don’t really seem consistent with BER and the ST elevation seems far too much to be BER but not able to rule out conclusively.
I’m going to put my money on Pericarditis but also unable to completely rule out STEMI or BER
LikeLiked by 1 person
Widespread ischaemia – what about something as basic as hypoxia secondary to lung CA?
LikeLiked by 1 person
Wide spread ST elevation I,II,II,avF, V3-V6 = pericarditis?
LikeLiked by 1 person
https://lifeinthefastlane.com/ecg-library/basics/pericarditis/
LikeLiked by 1 person
Good on you for having a go at commenting on the ECG as it is obviously a still daunting thing to do despite we are doing our best to make this forum free from any negative criticism.
And yes, your interpretation is certainly one of the differencials.
Can you think of any other pathologies?
In terms of your obs re biphasic T waves, do you think the T waves on V1 deflect both positively and negatively across the isoelectric line?
Please encourage others to post their guess as I can guarantee that it will not cost their job or reputation, lol 😄
LikeLike
I’ll have a stab at it… the STE in inferior aspects naturally suggests RCA occlusion, and the STE in anterior lateral aspects suggest Cx occlusion.
Of note the biphasic T waves have an occlusion style pattern similar to De Winters or Wellens in V1.
Overall the ECG suggests to me there’s a current infarct to the inferior and lateral aspects, but is progressing into a full occlusion of both LAD and RCA.
LikeLiked by 1 person